eHealth Africa (eHA) continues its close collaboration with Guinea’s Ministry of Health by contributing to their efforts to reform the country’s healthcare system, with supporting funds from The Paul G. Allen Ebola Program.
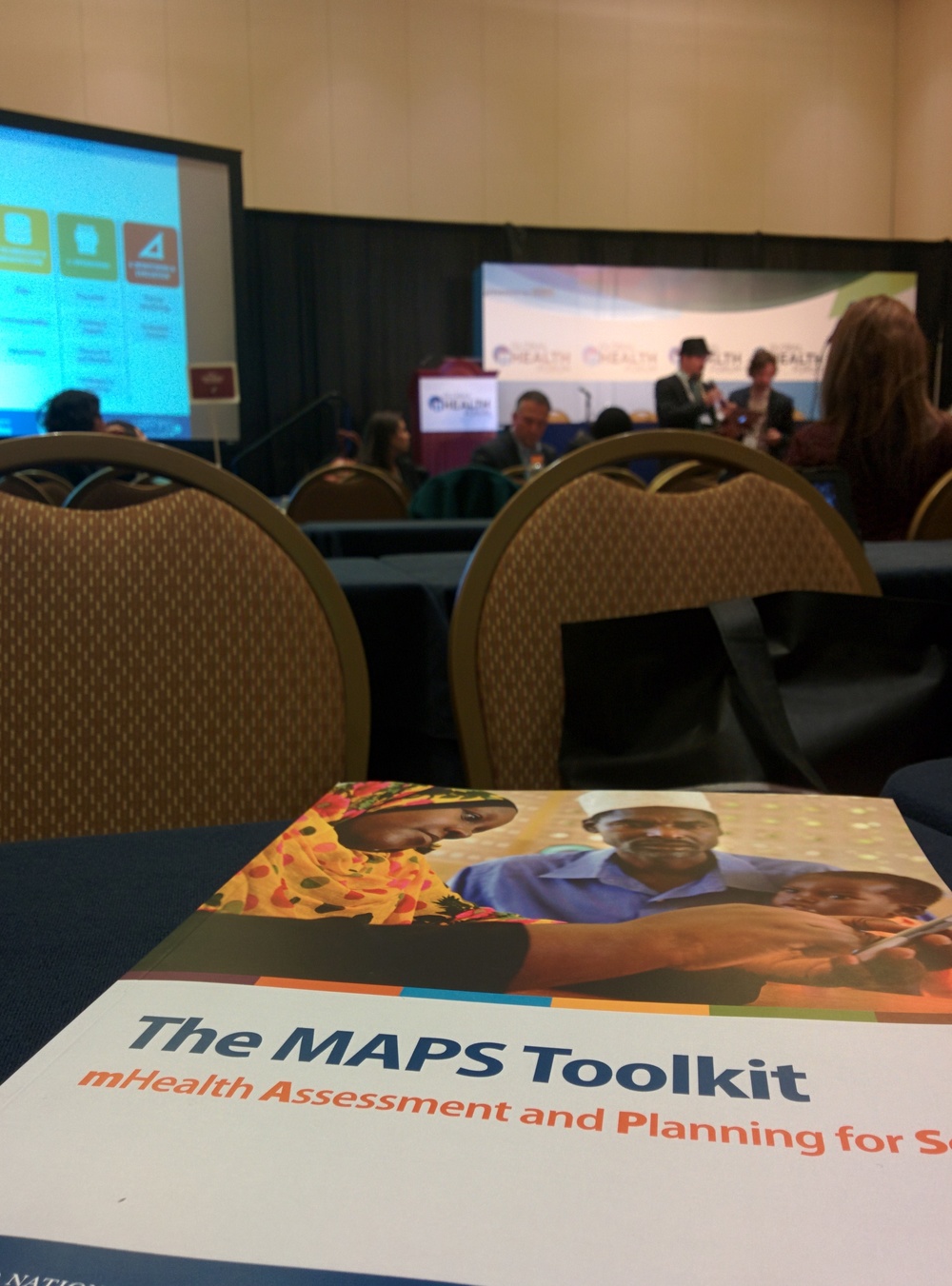
In January 2015, eHA launched Guinea Connect in the prefecture of Pita, by helping health facilities produce their very first digital monthly reports. Guinea Connect was designed by eHealth Africa's Berlin based Global Informatics Department and is being locally managed by eHA Guinea’s Information and Communication Technology team. Guinea Connect’s objectives are to incorporate data-sharing mechanisms and centralize health facility data from primary health care providers. The program will enhance the overall health systems communication and allow for rapid and effective decision making.
Guinea Connect is a not a stand alone system, it is one aspect of eHealth Africa's Integrated Community Health Post Pilot program, which was launched in September 2015 in the sub-prefecture of Timbi Tounni. The program covers eight districts in the sub-prefecture. Overall, the program is piloting the use of an eHealth data collection application, automating health facility monthly reports, creating a ministerial closed user group, and introducing an e-learning platform to community health workers. The platform will support Guinea’s Ministry of Health’s capacity building program for its agents.
The pilot program also entails refurbishing six Health Posts, building one Health Post, transforming the former health center building into a residential facility for center workers, and building a new suitable Health Center. eHA will temporarily support operations in all facilities and gradually hand over to a newly created Community Association, which will ensure sustainability. The association will be composed of members from existing community groups and the diaspora.
Local authorities, Ministry of Health officials, as well as the community members welcomed the program and the opportunity to work together with eHA in improving the area’s health system. In December 2015, community members had the opportunity to express their gratitude directly to the Paul G. Allen Ebola Program's Deputy Director Brennan Banks, who visited the project area.