By Joshua Ozugbakun & Emerald Awa- Agwu
In line with eHealth Africa’s quest to add more value to the states that we live and work in, the Polio Emergency Operations Centres are being rebranded to provide much more than administrative and coordination functions to the states.
“‘’All the work that eHA does is not for ourselves but to make our partners’ work better’’”
The Emergency Operating Centres (EOCs) were created by eHealth Africa and other partners such as U.S. Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), and Public Health England to serve as centers for the emergency management and response coordination of Polio and other infectious diseases in Nigeria. The EOCs are located in Abuja, Kano, Katsina, Sokoto, Kaduna, Borno, Bauchi, and Yobe states and during an outbreak, the EOCs serve as a central command and control facility responsible for carrying out the principles of emergency preparedness and emergency management.
After the establishment of the EOCs, eHealth Africa continues to support the center by ensuring that 24-hour electricity and internet access are available and that Technical/ Administrative Coordinators are on hand to ensure connectivity and the maintenance of the EOCs. However, this year, eHA decided that the Technical and Administrative Coordinators could be supporting the states in more ways. Here’s how:
Step 1: Capacity Building Workshop
eHealth Africa trained a total of 17 technical and admin coordinators from the 16th to 24th of April, 2018. This was the first step in the transition of eHA’s role in the EOCs from administrative to technical. The T/A Coordinators were trained on Geographical Information Systems (GIS), Analytics and Data Management.

Photo of Capacity Building Training
Step 2: 60- day Transition Phase
Following the successful conclusion of the capacity building workshop, the EOC technical support team (formerly the T/A coordinators) are undergoing a transition window during which they are expected to utilise the skills they had gained in their day to day activities at the EOCs. Some of these skills include:
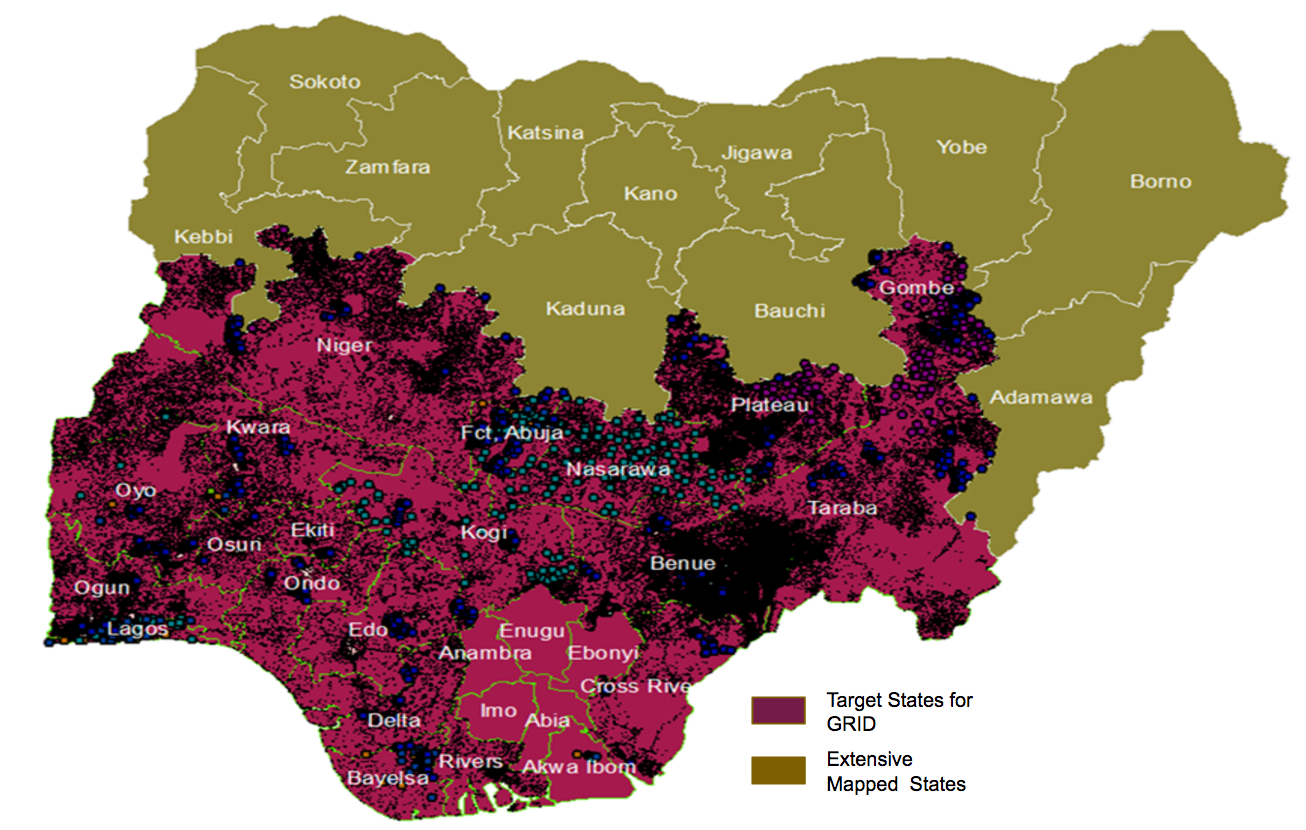
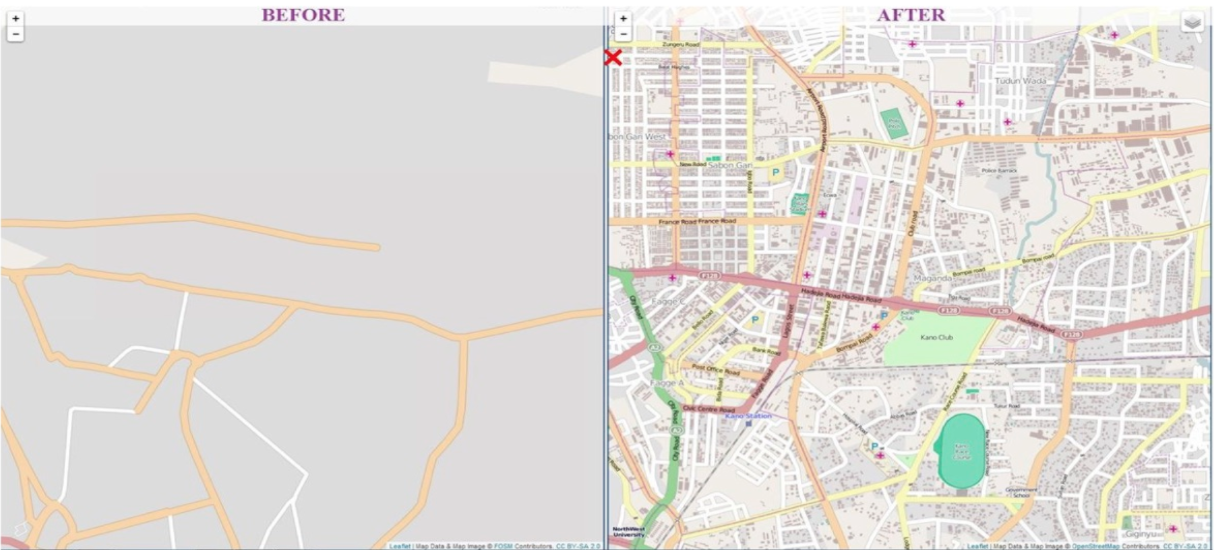
Creation of maps to support routine immunization and other micro-planning activities in the states
Acting as frontline brand ambassadors to showcase eHA solutions such as Logistics Management Information System (LoMIS) Suite, Vaccine Direct Delivery (VDD) etc.
This phase is intended to assess the abilities of the EOC technical support teams will be to use these skills; as well as to identify and address areas of growth or gaps in knowledge.
Eventually, the EOC technical support teams will be able to act as frontline representatives of eHealth Africa to the states and partners who utilize the EOCs where they are domiciled. They will be able to add more value to eHA as well by identifying more opportunities for business development.

Behold the new faces of the EOCs!