Written By Olajumoke Arinola & Nwanyibuife Obiako
eHealth Africa (eHA) is collaborating with the World Health Organization (WHO), Bill and Melinda Gates Foundation (BMGF), and Novel-T to scale up Acute Flaccid Paralysis (AFP) surveillance in Liberia, Sierra Leone, and Chad.

AFP surveillance remains a key indicator of the progress of polio eradication in Africa. Building on the success of the pilot of the mobile based Auto-Visual AFP Detection and Reporting (AVADAR) surveillance system in Nigeria, the project has been scaled up to strengthen surveillance by improving timely detection and reporting of suspected AFP cases in countries at risk of the re-emergence of the polio virus, and those most recently affected by the Ebola virus disease.
AVADAR has been operational since March of 2017 in the Liberian districts of Commonwealth, St. Paul, Careysburg, and Central Monrovia. It has also been used in the Sierra Leonean districts of Western Urban, Western Rural, Tonkolili, and Kono. More recently, Community Informants and Healthcare Workers (HCWs) were trained by eHA instructors on the use of the AVADAR app in Chad, making Chad the first francophone country utilizing AVADAR.
"In Chad, our team saw first hand the essence of integration of project planning with local context in terms of recruitment, training language, understanding health administrative levels, and the impact of country-specific regulations on logistics coordination and project success" - Olajumoke Arinola, Assistant Project Manager

Five weeks after its implementation in Sierra Leone, 4 AFP cases were detected out of the 41 suspected case alerts reported through the AVADAR. In Liberia, 6 AFP cases were detected out of the 89 suspected cases. After one week of implementation in Chad, 8 cases were reported and investigated with 1 confirmed to be an AFP case by Disease Surveillance and Notification Officers (DSNOs). Pre-implementation activities and partner coordination have commenced for other Lake Chad region countries, namely Cameroon and the Niger Republic.
In 2016, there were 3 new cases detected of wild poliovirus and circulating vaccine-derived poliovirus type 2 (cVDPV2) in Borno, a security-challenged state in northern Nigeria. This prompted the urgency to strengthen surveillance not only in Nigeria but across the entire Lake Chad region. In selecting specific local government areas and districts where AVADAR would be functional per country, WHO and the respective Ministries of Health (MoH) prioritized working in densely populated areas where AFP surveillance had been reportedly low.
[youtube=://www.youtube.com/watch?v=XAdFYmQ2oMo&w=640&h=480]
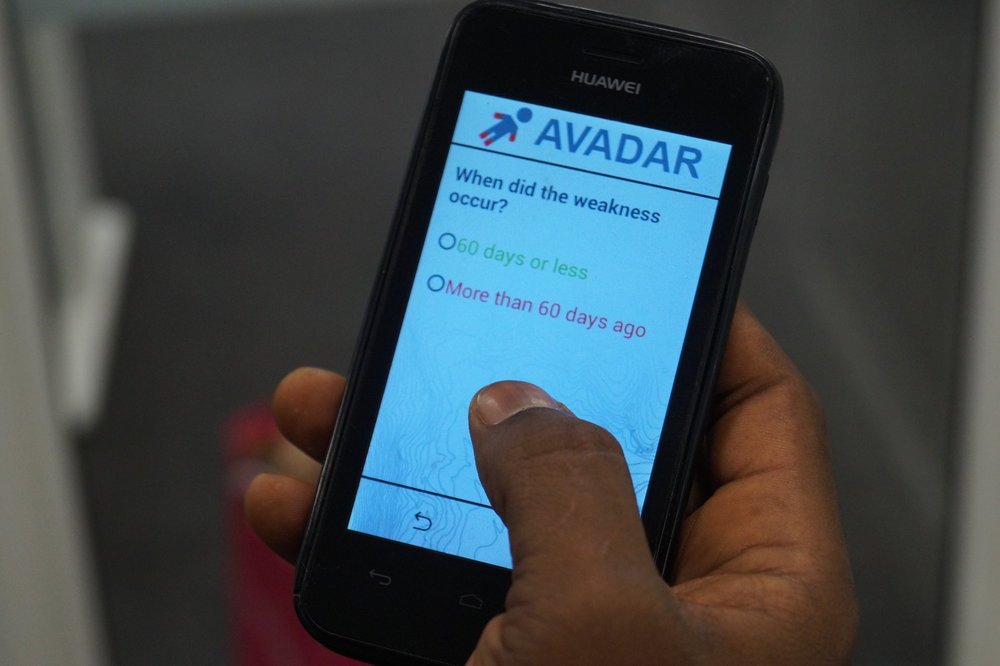
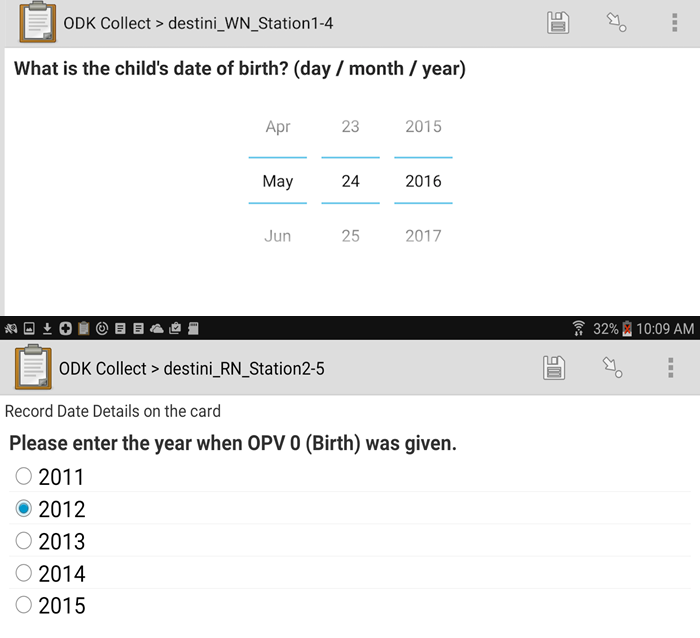
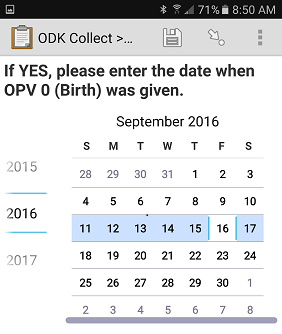
The AVADAR app has a 30-second video of a child with AFP symptoms embedded in it which reminds Community Informants and Healthcare Workers to report suspected cases weekly. In addition to English, the video has already been produced in the three major Nigerian languages (Hausa, Igbo, and Yoruba), major languages in Sierra Leone (Krio, Themne, Mende, and Kono), and French. To avoid ambiguity and to generate maximum impact, the AVADAR video was also voiced in Chadian Arabic with text translations in French for its implementation in Chad. This has increased the surveillance network in these countries through sensitization of traditional birth attendants, traditional healers, barbers, and other community residents on how to accurately detect and report suspected AFP cases.
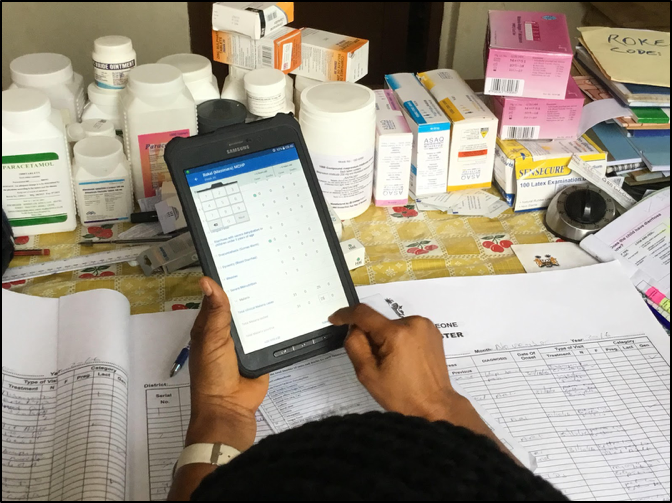
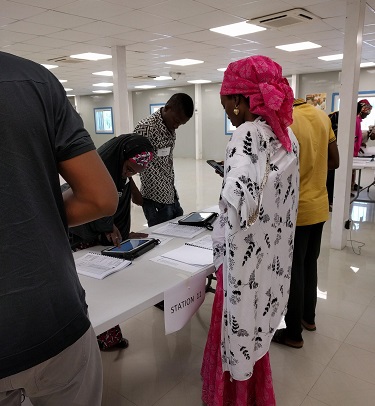
To date, eHA has distributed GPS-enabled mobile devices and solar chargers to over 2,000 Community Informants and Healthcare Workers in the four current AVADAR focus countries. eHA has also trained each mobile device recipient on the proper use of the phones and the AVADAR app. To ensure Community Informants were fully sensitized on how to detect and report suspected AFP cases through the app, participants were divided into small groups, with just 10-15 students per eHA instructor. Ample time was allocated to role plays and class demonstrations with the instructors communicating in the local language of the informants.
"Without eHA’s strategy of one facilitator to a group of 10 informants, these people (informants) wouldn’t have been able to use these phones and report AFP cases." - Dr. Faisal Shuaib, Executive Director, NPHCDA
eHA remains committed to working with Ministries of Health and other AVADAR implementing partners to strengthen AFP surveillance systems across Africa in order to end the spread of polio. Visit our website to find out more about our work strengthening West Africa’s disease surveillance systems.